The Role of Prolactin in the Body
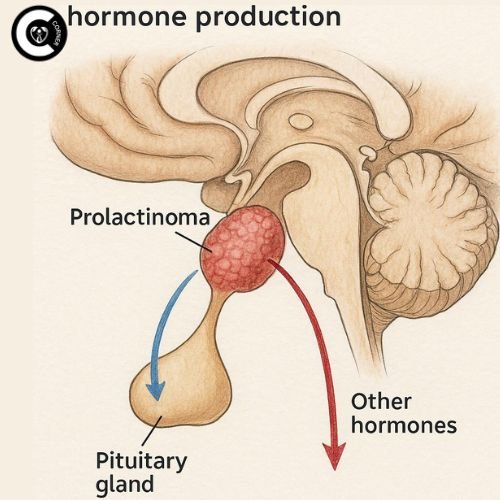
The pituitary gland, which is the size of a pea and is located near the base of the brain, makes prolactin. Its main job is to make breastfeeding women produce more milk. Prolactin also affects reproductive health by controlling the amounts of estrogen and testosterone. Prolactin levels are usually low in people who are not pregnant. When these levels go up too much, a disease called hyperprolactinemia occurs. This throws off the balance of sex hormones, which can cause symptoms including irregular periods, low libido, and infertility. High levels of prolactin can also mess with how bones break down and build up, which can raise the risk of osteoporosis over time.
Why Elevated Prolactin Matters
Hyperprolactinemia isn’t simply a problem with hormones; it’s a problem with the whole body. High levels of prolactin stop the body from making gonadotropin-releasing hormone (GnRH), which is necessary for women to ovulate and men to make sperm. The body can’t release luteinizing hormone (LH) and follicle-stimulating hormone (FSH) without GnRH, which stops reproductive activities. Long-term high levels can also cause bone density loss, long-term weariness, and mental health problems like anxiety or depression. Causes might be anything from benign pituitary tumors (prolactinomas) to drugs or thyroid problems. Early identification is very important to avoid long-term problems.
Recognizing the Symptoms of Hyperprolactinemia
Symptoms in Women
Women are more likely to identify hyperprolactinemia early since it has a direct effect on their menstrual health. Higher levels of prolactin can stop ovulation, which can cause periods to be erratic or stop altogether (amenorrhea). For instance, a woman can have cycles that skip months or get unexpectedly light. Galactorrhea, which is a milky discharge from the nipple that isn’t connected to breastfeeding, is a common sign that can be confusing or embarrassing. Low estrogen levels can induce vaginal dryness, which can make sex uncomfortable and put a strain on relationships. High prolactin stops eggs from being released, which makes it hard to get pregnant without therapy. This is a big problem for people who want to have children.
Symptoms in Men
Men with hyperprolactinemia often have symptoms that are less obvious and take longer to show up. When testosterone levels drop, it can cause erectile dysfunction (ED) and a big drop in libido. Some men get gynecomastia, which is when breast tissue grows because there is too much testosterone and not enough estrogen. Over time, sperm production goes down, which can lead to a low sperm count or poor motility. A lot of guys think these changes are just stress-related, so they don’t get diagnosed until they have trouble getting pregnant.
Shared Symptoms
Chronic weariness can happen to people of both sexes, and it is commonly confused with burnout. If a pituitary tumor presses on nearby brain tissue, headaches are prevalent. Low estrogen or testosterone levels can lower bone density, which makes fractures more likely. For example, a 40-year-old with untreated hyperprolactinemia might have bones that are as strong as those of a 70-year-old. These consequences on the whole body show how important it is to treat the problem as a whole.
What Causes Hyperprolactinemia?
Prolactinomas: The Leading Cause
Prolactinomas are tumors in the pituitary gland that make too much prolactin. They make up 40% of all pituitary tumors and are sorted by size:
- Microadenomas (less than 10 mm): These tumors are often asymptomatic and are found by chance during brain imaging.
- Macroadenomas (>10 mm): These bigger tumors can stress on the optic nerve, which can make you lose your eyesight or see double. They can also cause bad headaches or make other pituitary processes worse, like making hormones for the thyroid or adrenal glands.
Medication-Induced Hyperprolactinemia
Some medicines mess with dopamine, a neurotransmitter that usually stops prolactin from being released. Some examples are:
- Antidepressants (SSRIs): fluoxetine or sertraline.
- Antipsychotics: haloperidol or risperidone.
- Anti-Emetic: Metoclopramide.
A lot of mental patients take these drugs, which are a common cause of hyperprolactinemia.
Other Contributing Factors
- Hypothyroidism: When the thyroid gland isn’t working properly, it makes more thyrotropin-releasing hormone (TRH), which makes prolactin work.
- Chronic kidney disease: When the kidneys don’t work right, they don’t eliminate prolactin from the blood as well.
- Injuries to the chest wall: Burns, shingles, or surgery can irritate nerves in the chest.
which might make the body think it’s breastfeeding and raise prolactin levels.
Idiopathic hyperprolactinemia is when no cause can be found in 30% of cases.
Diagnosing Hyperprolactinemia
Blood Tests and the “Hook Effect”
The first step is a fasting blood test because eating or being stressed can raise prolactin levels for a short time. The normal ranges are:
- Women: less than 25 ng/mL
- For men: <20 ng/mL
If your levels are more than 200 ng/mL, you probably have a prolactinoma. But when levels are really high (more than 500 ng/mL), they might break lab equipment and give a misleadingly low value, which is called the “hook effect.” This problem goes away when the blood sample is diluted.
Imaging and Advanced Diagnostics
An MRI of the pituitary gland is the best way to find tumors. A T1-weighted MRI with contrast dye, for instance, makes even the smallest microadenomas stand out. More tests are:
- Tests of thyroid function: To make sure youon’t have hypothyroidism.
- Pregnancy test: For women, to rule out natural sources of elevated prolactin.
- Tests of kidney and liver function are conducted to determine whether metabolic reasons are responsible.
Hyperprolactinemia and Fertility: Breaking the Link
How High Prolactin Disrupts Reproduction
High levels of prolactin stop GnRH, the hormone that makes LH and FSH. This stops ovulation in women, which can cause irregular cycles or amenorrhea. For instance, a woman with 100 ng/mL of prolactin may stop ovulating altogether. Low testosterone lowers the number of sperm and how well they move in men. Couples who have been trying to get pregnant for more than a year should think about getting a prolactin test.
Restoring Fertility with Treatment
- Dopamine agonists: Including cabergoline (0.5–2 mg/week) or bromocriptine (2.5–15 mg/day), decrease tumors and bring prolactin levels back to normal in 80–90% of patients. A lot of women start ovulating again within a few weeks.
- IVF: For people who don’t respond to medicine, in vitro fertilization gets around problems with ovulation.
- Surgery: Transsphenoidal resection takes out big tumors that are putting pressure on important structures.
Treatment Options for Hyperprolactinemia
Medication Management
- Cabergoline: A dopamine agonist that you take twice a week. It works quite well, but you need to watch for unusual adverse effects like thickening of the heart valves at large doses.
- Bromocriptine: Older and less well-tolerated because it makes you sick, but safer during pregnancy.
Surgical Interventions
People only have surgery on macroadenomas that don’t respond to medicine or that make them lose their vision. The transsphenoidal method, which goes through the nose, cuts down on recuperation time. The size of the tumor affects the success rate. For example, microadenomas have a 90% remission rate.
Lifestyle Adjustments
- How to deal with stress: Yoga or meditation can suppress cortisol levels, which can make prolactin levels worse.
- Don’t stimulate the chest: Wearing tight bras or checking your nipples a lot can raise prolactin levels by accident.
- Take care of any underlying problems: Thyroid hormone replacement for people with hypothyroidism.
Living with Hyperprolactinemia
Also Read: How To Boost FSH Level Naturally
Bone Health Strategies
Loss of estrogen or testosterone speeds up bone loss. To keep an eye on her bone density, a 50-year-old woman with hyperprolactinemia may need dual-energy X-ray absorptiometry (DEXA) scans. Taking calcium (1,200 mg/day) and vitamin D (800–1,000 IU/day) supplements, coupled with weight-bearing workouts like walking, might help you stay strong.
Pregnancy and Hyperprolactinemia
Most women quit taking dopamine agonists when they get pregnant because prolactin levels naturally rise during pregnancy. Hormonal changes, on the other hand, can make macroadenomas grow, thus they need to be watched with an MRI. If you require medicine while you’re pregnant, bromocriptine is safer.
Mental Health Support
Hormonal imbalances and infertility might make you feel anxious or depressed. Cognitive-behavioral therapy (CBT) and support groups can help you deal with your problems. A study from 2022, for example, found that 35% of people with hyperprolactinemia said their mental health was better after joining peer support groups
The Future of Hyperprolactinemia Care
Emerging Therapies
- Kisspeptin therapy: This hormone directly activates GnRH, which gives women who don’t respond to dopamine agonists hope.
- Targeted drug delivery: Nanoparticle-based devices may send medicine straight to pituitary tumors, which could lower side effects.
Genetic Research
Genetic Research Studies are finding gene mutations (such as PRLR or AIP genes) that are associated with idiopathic instances. This opens the door for personalized therapy.
[…] Also Read: Effect Of Hyperprolactinemia On Fertility […]
[…] Also Read: How High Prolactin Levels Impact Conception […]